N35) History of seizures and developmental delay
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with seizures.
- Review the DDx considerations in a patient with seizures.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with seizures.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
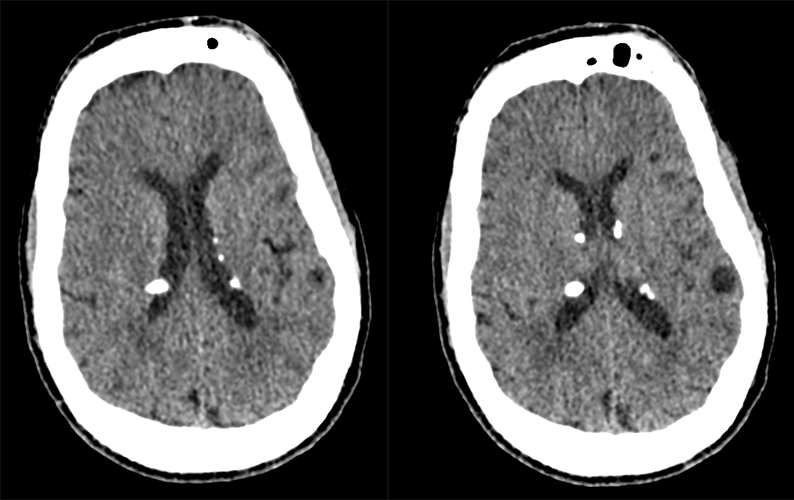
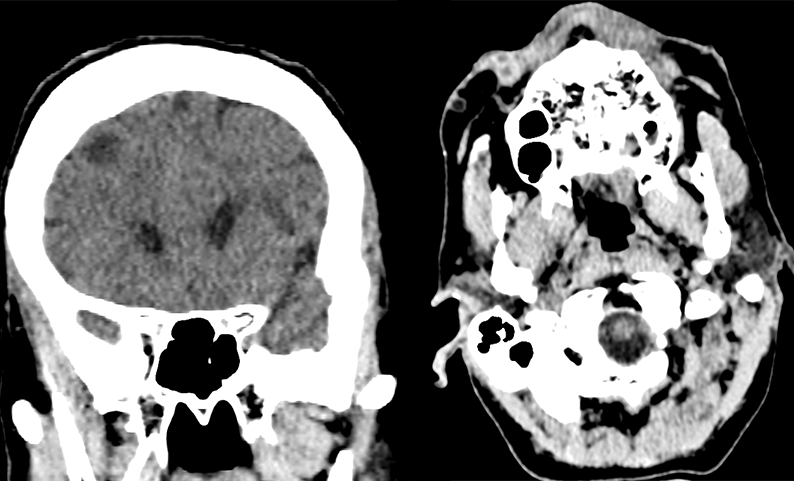
CT Brain without IV contrast
What is the location of the calcified lesions?
There are otherwise no other findings.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
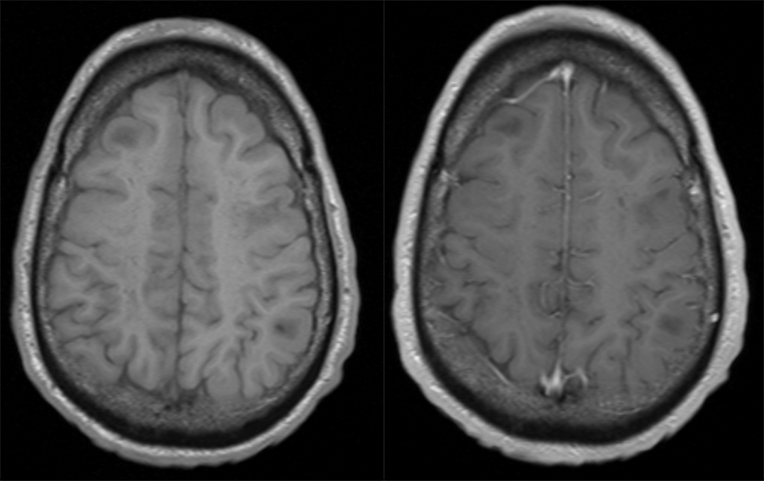
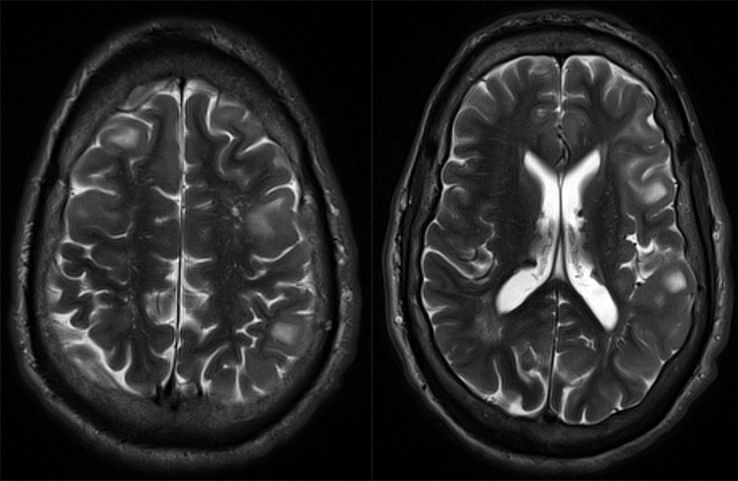
MRI brain with and without contrast.
The subcortical nodules enhance following contrast administration.
On T2, the subcortical nodules are:
Watch our video
Third Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Tuberous sclerosis complex (TSC), also known as Bourneville disease, is a genetic disorder that affects multiple organ systems, characterized by the development of tumors of the embryonic ectoderm. It is rare, affecting approximately 1 in 10,000 people and is inherited in an autosomal dominant pattern. TSC is caused by loss-of-function germline mutations in the tumor suppressor genes TSC1 or TSC2.
- Although the classic clinical triad of seizures, intellectual disability, and facial angiofibromas (Vogt triad) is associated with TSC, it is seen in less than 50% of cases. The diagnostic criteria for TSC has been updated to include a pathogenic mutation of TSC1 or TSC2 along with the presence of two major features or one major feature with two minor features.
- Major features of TSC include hypomelanotic macules, angiofibromas or fibrous cephalic plaques, ungual fibromas, Shagreen patches, multiple retinal hamartomas, cortical dysplasias, subependymal nodules, subependymal giant cell astrocytomas (SEGAs), lymphangioleiomyomatosis (LAM), cardiac rhabdomyomas, and angiomyolipomas (AML).
- Minor features include "Confetti" skin lesions, dental enamel pits, intraoral fibromas, retinal achromic patches, multiple renal cysts, and nonrenal hamartomas.
- Radiologists have a crucial role in the early diagnosis and lifelong follow-up of patients with TSC-related manifestations. Without frequent monitoring and intervention, TSC can result in significant morbidity and mortality. Radiologists can help identify and monitor the development of TSC-associated tumors and other abnormalities, enabling timely intervention to improve patient outcomes.
Socioeconomic Factors:
- Early recognition and diagnosis of TSC remains a challenge due to its varying, multisystem presentation. As in this case, patients who are uninsured or have suboptimal access to comprehensive healthcare have significant delay in their diagnoses and can suffer significant physical, financial, and emotional costs.
- The psychosocial impact of a TSC diagnosis is significant. A recent study examining the psychosocial burden on patients and their families found that TSC has profoundly negative impacts on patients’ careers, relationships with their families and caregivers, and mental health, with a high incidence of associated anxiety and depression.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}